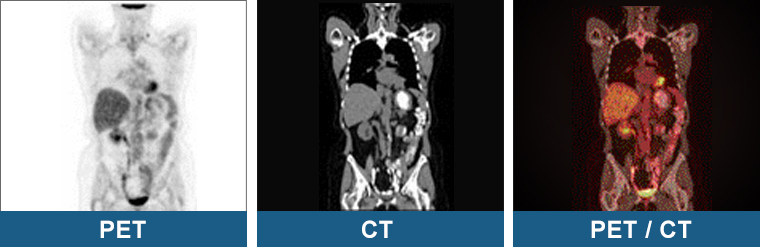
Positron emission tomography (PET) is a nuclear medicine imaging modality that can be used to create whole body images of physiological processes. In contrast, CT and MR create images of anatomy. PET/CT is a newly developed technology that combines a fully diagnostic PET/CT scanner with a fully diagnostic CT scanner that can simultaneously create complementary images of physiology and anatomy.
For many diseases, most notably cancer, PET/CT can detect changes in physiology 6 months to a year before CT or MR can detect changes in anatomy. This allows PET/CT to detect disease in normal sized structures as well as to detect early response to therapy.
Furthermore, PET/CT can accurately detect disease in regions where post therapeutic change has distorted anatomy.
Currently, almost all PET/CT scans are performed using the radiopharmaceutical F-18 fluorodeoxyglucose (FDG). F-18 is a positron emitter with a two hour half-life. FDG is a glucose analog that is used to create images of glucose metabolism. For an excellent discussion about the normal variants of FDG uptake please see Shreve 1999.
Clinical indications for PET/CT include oncology, neurology and cardiology. In oncology, rapidly growing neoplasms fuel their growth with glucose making FDG PET/CT the most sensitive and specific modality for imaging them. In Alzheimer’s disease, FDG PET/CT can detect disease specific reductions in neuronal activity long before it can be detected with any other test. In cardiology, FDG PET/CT can accurately assess myocardial viability in hypo-perfused regions of the myocardium.
Compared to CT or MR, the overall the sensitivity and specificity of PET/CT is typically at least 10% higher. The peer-reviewed scientific literature shows that PET/CT can lead to significant changes in patient management at least 40% of the time. PET/CT is well tolerated by most patients and is routinely reimbursed by most insurance companies. For many indications, PET/CT is rapidly becoming part of standard care.
